Key points: Acute isocapnic hypoxia elicits lasting sympathoexcitation that does not correspond to parallel changes in vascular tone, suggesting blunted sympathetic transduction. Signal-averaging techniques track the magnitude and temporal cardiovascular responses following integrated muscle sympathetic nerve activity (MSNA) burst and nonburst cardiac cycles; however, this does not fully characterize the effects of sympathetic action potential (AP) activity on blood pressure control. We show that hypoxia blunts the sympathetic transduction of mean arterial pressure (MAP) following synchronous APs that form integrated MSNA bursts and that sympathetic transduction of MAP remains attenuated into early recovery. At rest, asynchronous APs attenuate the reduction in MAP compared to cardiac cycles following no AP activity, thus asynchronous sympathetic APs appear to contribute to the neural regulation of blood pressure. The results advance our understanding of sympathetic transduction of arterial pressure during and following exposure to acute isocapnic hypoxia in humans.
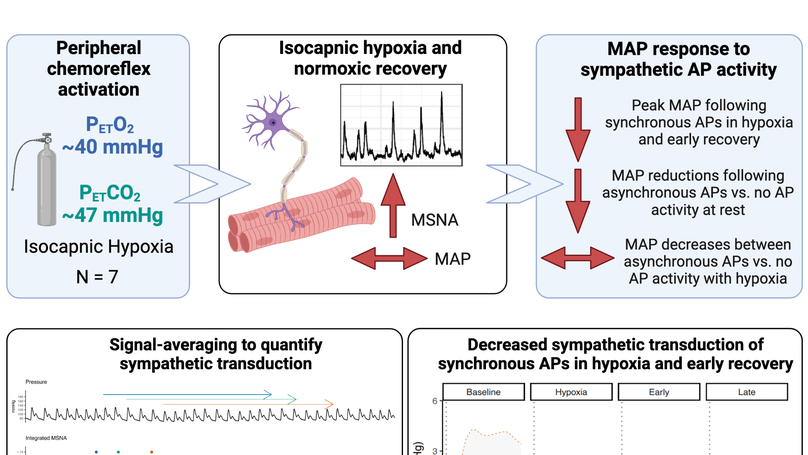
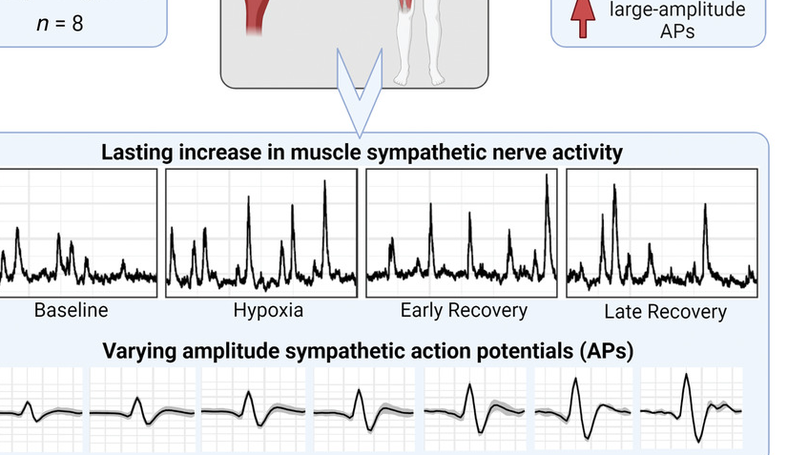
Abstract: Post-hypoxia sympathoexcitation does not elicit corresponding changes in vascular tone, suggesting diminished sympathetic signalling. Blunted sympathetic transduction following acute hypoxia, however, has not been confirmed and the effects of hypoxia on the sympathetic transduction of mean arterial pressure (MAP) as a function of action potential (AP) activity is unknown. We hypothesized that MAP changes would be blunted during acute hypoxia but restored in recovery and asynchronous APs would elicit smaller MAP changes compared to synchronous APs. Seven healthy males (age: 24 (3) yrs; BMI: 25 (3) kg/m2 ) underwent 20-min isocapnic hypoxia (PET O2 : 47 (2) mmHg) and 30-min recovery. Multi-unit microneurography (muscle sympathetic nerve activity; MSNA) and continuous wavelet transform with matched mother wavelet was used to detect sympathetic APs during baseline, hypoxia, early (first 7-min), and late recovery (last 7-min). AP groups were classified as synchronous APs, asynchronous APs (occurring outside a MSNA burst), and no AP activity. Sympathetic transduction of MAP was quantified using signal-averaging, with ΔMAP tracked following AP group cardiac cycles. Following synchronous APs, ΔMAP was reduced in hypoxia (+1.8 (0.9) mmHg) and early recovery (+1.5 (0.7) mmHg) compared to baseline (+3.1 (2.2) mmHg). AP group-by-condition interactions show that at rest asynchronous APs attenuate MAP reductions compared to no AP activity (-0.4 (1.1) vs. -2.2 (1.2) mmHg, respectively), with no difference between AP groups in hypoxia, early, or late recovery. Sympathetic transduction of MAP is blunted in hypoxia and early recovery. At rest, asynchronous sympathetic APs contributes to neural regulation of MAP by attenuating nadir pressure responses. Abstract figure legend Seven healthy men underwent 20-min isocapnic hypoxia and 30-min recovery. The study tested the hypotheses that hypoxia would blunt the sympathetic transduction of mean arterial pressure (MAP) following synchronous AP activity and that asynchronous APs would elicit smaller ΔMAP compared to synchronous APs. All sympathetic APs were detected and extracted from the filtered MSNA neurogram using a continuous wavelet transform with matched mother wavelet. AP groups were classified as synchronous (with MSNA burst), asynchronous (outside MSNA burst), and no AP activity. An effect of condition showed that following synchronous APs, ΔMAP was reduced in hypoxia and early recovery compared to baseline. AP group-by-condition interactions revealed that asynchronous APs attenuate MAP reductions compared to no AP activity under resting conditions. Our findings demonstrate that sympathetic transduction of MAP is blunted in hypoxia and remains diminished into early recovery. At rest, asynchronous AP activity contributes to MAP regulation by attenuating pressure reductions.